
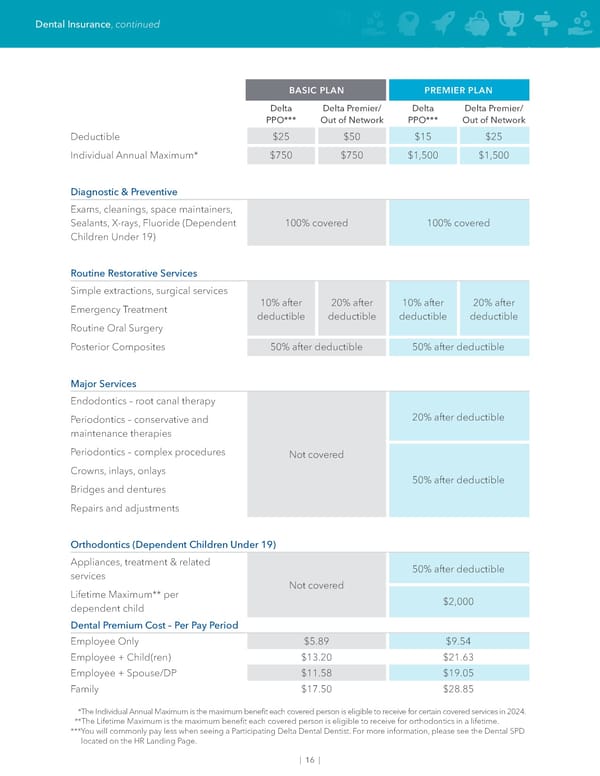
| 16 | Dental Insurance, continued BASIC PLAN PREMIER PLAN Delta PPO*** Delta Premier/ Out of Network Delta PPO*** Delta Premier/ Out of Network Deductible $25 $50 $15 $25 Individual Annual Maximum* $750 $750 $1,500 $1,500 Diagnostic & Preventive Exams, cleanings, space maintainers, Sealants, X-rays, Fluoride (Dependent Children Under 19) 100% covered 100% covered Routine Restorative Services Simple extractions, surgical services 10% after deductible 20% after deductible 10% after deductible 20% after deductible Emergency Treatment Routine Oral Surgery Posterior Composites 50% after deductible 50% after deductible Major Services Endodontics – root canal therapy Not covered 20% after deductible Periodontics – conservative and maintenance therapies Periodontics – complex procedures 50% after deductible Crowns, inlays, onlays Bridges and dentures Repairs and adjustments Orthodontics (Dependent Children Under 19) Appliances, treatment & related services Not covered 50% after deductible Lifetime Maximum** per dependent child $2,000 Dental Premium Cost – Per Pay Period Employee Only $5.89 $9.54 Employee + Child(ren) $13.20 $21.63 Employee + Spouse/DP $11.58 $19.05 Family $17.50 $28.85 *The Individual Annual Maximum is the maximum benefit each covered person is eligible to receive for certain covered services in 2024. **The Lifetime Maximum is the maximum benefit each covered person is eligible to receive for orthodontics in a lifetime. *** You will commonly pay less when seeing a Participating Delta Dental Dentist. For more information, please see the Dental SPD located on the HR Landing Page.
 Team Members Guide Page 17 Page 19
Team Members Guide Page 17 Page 19